
When we talk about HIV prevention, the conversation often revolves around policies, medical breakthroughs, and statistics. All of these are important. But during a recent study visit to London, I was reminded that the most powerful tool in prevention is often something far simpler: trust.
Trust is what allows someone to walk into a clinic and ask for an HIV test. It’s what makes a person feel comfortable asking questions about PrEP or talking openly about their sexual health or drug use. Without trust, even the best prevention strategies struggle to reach the people who need them most.
Through the SCOPE study visit, I had the opportunity to visit the Africa Advocacy Foundation (AAF) in London, a community-led organisation working to improve health and wellbeing among African diaspora communities. What I experienced during that visit stayed with me long after I returned home to Sweden.
Because in many ways, the conversations happening in London felt very familiar.
Working with Communities in Malmö
I work in Malmö as a Community Health Educator, focusing on HIV combination prevention and sexual and reproductive health.
Much of my work involves engaging with communities that often face barriers when accessing healthcare and prevention services. These include migrants, sex workers, transgender people, gay and bisexual men, other men who have sex with men, people who inject drugs, and individuals involved in chemsex.
Many people within these communities navigate stigma, discrimination, or structural barriers that make accessing healthcare more complicated than it should be.
My role is partly about providing information — explaining HIV testing, treatment, and prevention tools like PrEP. But just as importantly, it’s about creating spaces where people feel safe enough to ask questions and talk openly about topics that are often surrounded by silence or judgment.
Over time, I’ve learned that prevention work is rarely just about health information. It’s about relationships, trust, and understanding the realities of people’s lives.
That’s why learning from organisations working with similar communities in other countries is so valuable.
Visiting the Africa Advocacy Foundation
The Africa Advocacy Foundation is widely recognised in the UK for its community-driven approach to health promotion. Their programmes focus on HIV prevention, sexual and reproductive health, stigma reduction, and improving health literacy within African and minority communities.
But what makes their work particularly powerful is that it is deeply rooted in the community itself.
Many of the people delivering the programmes share cultural backgrounds and lived experiences with the communities they serve. This creates a level of connection and trust that traditional health messaging often struggles to achieve.
During my visit, I joined a small community discussion about sexual health and HIV prevention. What struck me immediately was the atmosphere.
The conversation felt open and relaxed. People asked questions freely. Experiences were shared honestly. Topics like HIV testing and prevention tools such as PrEP came up naturally in the discussion rather than being presented in a formal or clinical way.
It didn’t feel like a lecture or a workshop.
It felt like a conversation among people who trusted each other.
And it was clear that this level of openness didn’t appear overnight. It was the result of long-term engagement, cultural understanding, and consistent presence within the community.
As I listened to the discussion, I couldn’t help noticing how many of the challenges being described sounded familiar.
Stigma around HIV. Limited awareness of prevention tools. Cultural barriers to discussing sexuality and sexual health.
These are challenges I see regularly in my work with migrant communities in Sweden.
Three Lessons That Stayed With Me
1.Prevention Starts with Trust
One of the strongest impressions I took from the visit was how central trust is to prevention work.
At AAF, trust has been built through long-term relationships with the community. Because of this, people feel comfortable approaching staff and volunteers to ask questions or seek support.
This makes conversations about HIV testing, sexual health, or prevention tools like PrEP much easier to have.
It was a powerful reminder that prevention is not only about sharing information.
It’s about creating the kind of relationships where people feel safe enough to talk.
2.Peer Educators Make Prevention Real
Another thing that stood out was the role of peer educators.
Community members themselves are involved in sharing information about HIV testing, treatment, and prevention. Because they come from the same communities, they can speak about these issues in ways that feel relatable and grounded in real life.
One peer educator explained that sometimes sharing personal experiences can have more impact than statistics.
When someone talks about their own journey with testing or prevention, it makes the information feel real and relevant.
For communities that experience stigma or marginalisation — whether related to migration status, sexuality, gender identity, or drug use — this kind of peer support can be incredibly powerful.
In many ways, this mirrors the peer-led outreach work we also use in Malmö.
Seeing it in action in another context reinforced how important it is to continue strengthening these approaches.
3.Community Organisations Can Bridge the Gap to Healthcare
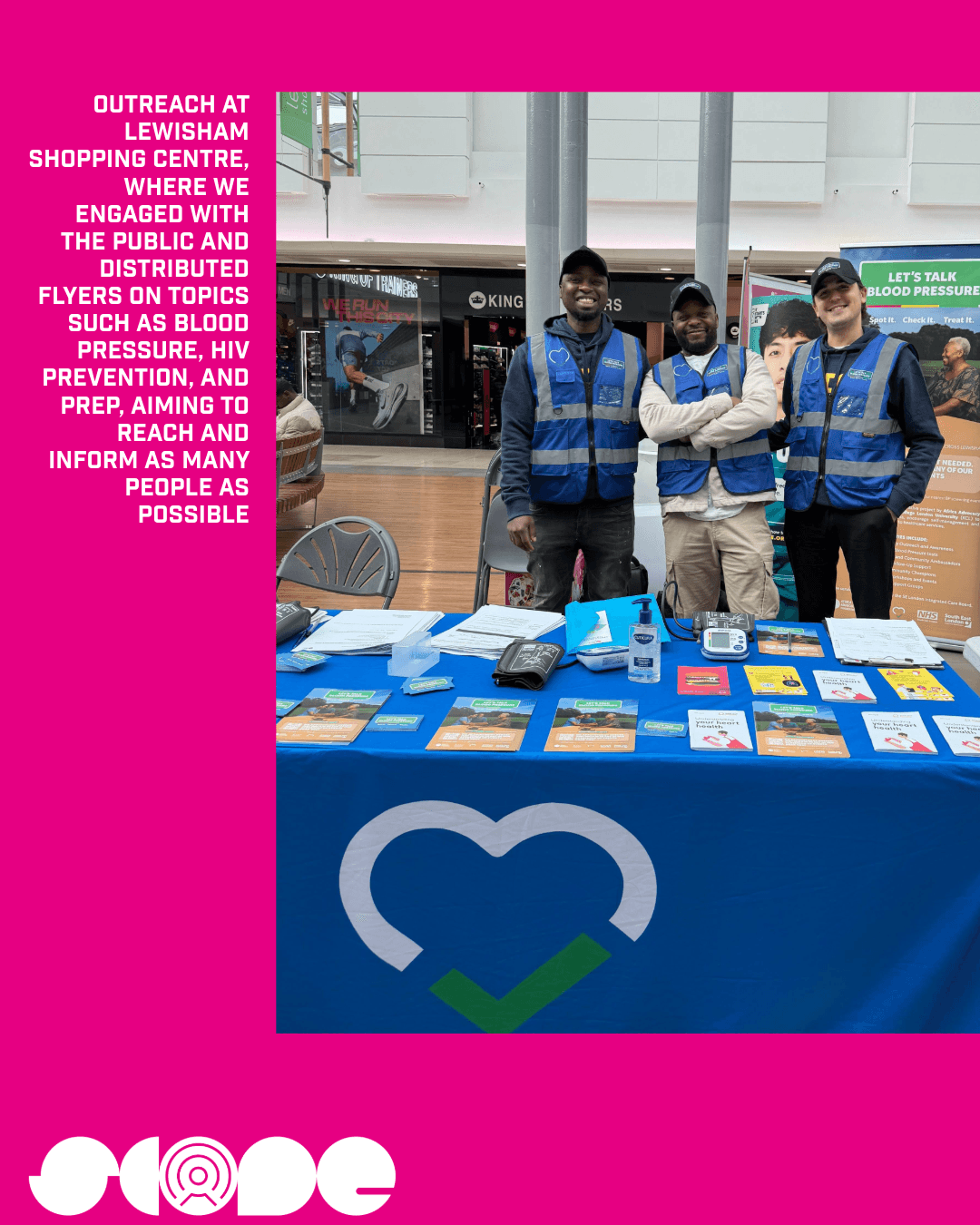
A third important lesson was the role community organisations can play in connecting people to healthcare services.
AAF works closely with healthcare providers and institutions connected to the UK’s national health system. These partnerships allow them to guide community members toward HIV testing, treatment, PrEP programmes, and sexual health clinics when needed.
For many people, community organisations are often the first point of trust.
They can help people navigate healthcare systems that might otherwise feel unfamiliar, intimidating, or inaccessible.
This kind of collaboration between grassroots organisations and health services is essential if prevention efforts are going to reach everyone.
Bringing the Learning Back to Malmö
Since returning from the study visit, I’ve been reflecting on how these lessons can strengthen the work we do in Malmö.
One area I want to continue developing is peer-led engagement within the communities we work with. Empowering community members to act as educators and advocates can help expand access to reliable information and reduce stigma around HIV.
I’m also thinking about how we can continue improving culturally responsive outreach, particularly when working with migrant communities where conversations around HIV, sexuality, or drug use may still feel sensitive.
Another priority is strengthening partnerships with healthcare providers and organisations working in sexual health and harm reduction. Strong collaboration makes it easier for people to move from information to actual access — whether that means testing, treatment, PrEP, or other support services.
The visit also opened the door to new professional connections with the African Advocacy Foundation. I hope this exchange of ideas continues, because learning from each other across countries can make all of our work stronger.
Looking Ahead
HIV prevention is most effective when communities themselves are placed at the centre of the response.
This visit reminded me how powerful community-led organisations can be in reaching people who might otherwise remain disconnected from healthcare systems.
By sharing experiences and learning across borders, we can adapt new ideas and continue improving how prevention work is done locally.
As I returned to Malmö, one thought stayed with me:
When communities lead the conversation about health, prevention becomes more than information — it becomes something people trust.
Denis Kolasinac
Noaks Ark Mosaik – Community Educator



EATG’s SCOPE project aims to strengthen the skills and knowledge of community health workers, advocates and researchers in the field of HIV combination prevention. It focuses on communities that are inadequately served by policies and programmes.
About the study trips
The SCOPE project provided two individual study trips for community health workers and advocates involved in HIV combination prevention service delivery in the WHO European region to carry out individual site visits to local community-based/led organisations.
Study trips provided the opportunity for community health workers and advocates in the area of HIV prevention to:
- Learn from peers about innovative, inclusive, and integrated HIV prevention services that can be adapted to their local setting
- Establish and/or strengthen partnerships with a host organisation(s).
The SCOPE project has been developed by the EATG and was made possible through a grant from ViiV Healthcare Europe Ltd.

Get involved
Are you living with HIV/AIDS? Are you part of a community affected by HIV/AIDS and co-infections? Do you work or volunteer in the field? Are you motivated by our cause and interested to support our work?
Subscribe
Stay in the loop and get all the important EATG updates in your inbox with the EATG newsletter. The HIV & co-infections bulletin is your source of handpicked news from the field arriving regularly to your inbox.